Weitz - The Coagulation Cascade: Review of Physiology and Clinical Applications - Figure 3
Coagulation Simplified
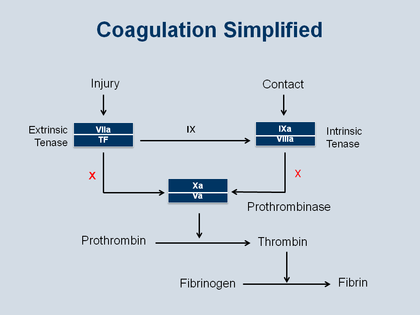
This Figure presents a coherent schematic of the coagulation cascade, in order to simplify all the factors with Roman numerals and highlight 3 activation complexes: extrinsic tenase on the left-hand side, intrinsic tenase on the right-hand side, converging on prothrombinase in the center of the Figure
Each of these complexes is built around an enzyme component:
• in the case of extrinsic tenase the enzyme component is factor VIIa
• in the case of intrinsic tenase the enzyme component is factor IXa
• in the case of prothrombinase the enzyme component is factor Xa
– with the enzyme component in the top part of each of the 3 boxes and the cofactor involved in these enzyme complexes in the lower part of the boxes:
• the cofactor for extrinsic tenase is tissue factor
• the cofactor for intrinsic tenase is factor VIIIa
• the cofactor for prothrombinase is factor Va
The way these complexes work is that they assemble on the surface of an activated cell. So think about the platelet as that surface: the activated platelet brings together the cofactor or/and the enzyme and then activate a subsequent clotting enzyme.
In the case of extrinsic tenase, that activated cell might be the subendothelial cell that is exposed at the site of entry and that now is expressing tissue factor on its surface. The enzyme binds to that tissue factor, factor VIIa, and that starts the whole process. So the factor VIIa–tissue factor (or extrinsic tenase) complex is the “spark” that was mentioned above. It is activated by injury, as shown in the upper left-hand side of the Figure, and that factor VIIa–tissue factor complex then activates factor X and the Xa. Factor Xa then binds to factor Va to form the prothrombinase complex, the prothrombinase complex then converts prothrombin to thrombin, and finally the thrombin converts soluble fibrinogen into insoluble fibrin.
This process may be amplified in several ways. Extrinsic tenase (the factor VIIa–tissue factor complex) also activates factor IX and the factor IXa then assembles into intrinsic tenase (as shown in the upper right-hand side of the Figure) to generate more factor Xa and more prothrombinase. The thrombin that is formed as a result of prothrombinase conversion of prothrombin to thrombin can then feed back to activate factor V, factor VIII, and factor XI, which are in the contact pathway to generate more intrinsic tenase, prothrombinase, and thrombin, respectively.
So from a tiny spark – ie, the site of injury – tissue factor is exposed and a whole series of reactions then results that end in thrombin generation. This burst of thrombin results in rapid fibrin formation, and this whole system is designed to form a hemostatic plug and seal the hole in a vessel. The problem is that if this occurs within the vessel, that fibrin–platelet network can seal up the vessel lumen and block blood flow, which then may result in a heart attack or stroke.
The upper right-hand of Figure 3 shows the intrinsic tenase and at the start of the contact pathway. The contact pathway begins the involvement of factor XII, factor XI, and their cofactors. This pathway is not shown here in detail because in most instances that pathway is not so important. However, in certain circumstances the contact pathway may be important for activation of clotting – as, for example, in the situation of patients who have mechanical heart valves or stents or some other medical device – because the artificial surface of these medical devices can trigger factor XII activation and initiate clotting through the contact pathway.
So in sum, in the case of tissue injury or vascular injury, extrinsic tenase is the initiator of the coagulation cascade, but for blood contacting devices it is the contact pathway initiation through the intrinsic tenase pathway. The bottom of Figure 3 illustrates that thrombin is critical for the conversion of soluble fibrinogen to fibrin, and fibrin then polymerizes to form the mesh work and the major protein component of the clot. Weitz JI. Am J Med 2013; published on-line at http://education.amjmed.com/00000.