Won - Figure 51
Summary (Continued)
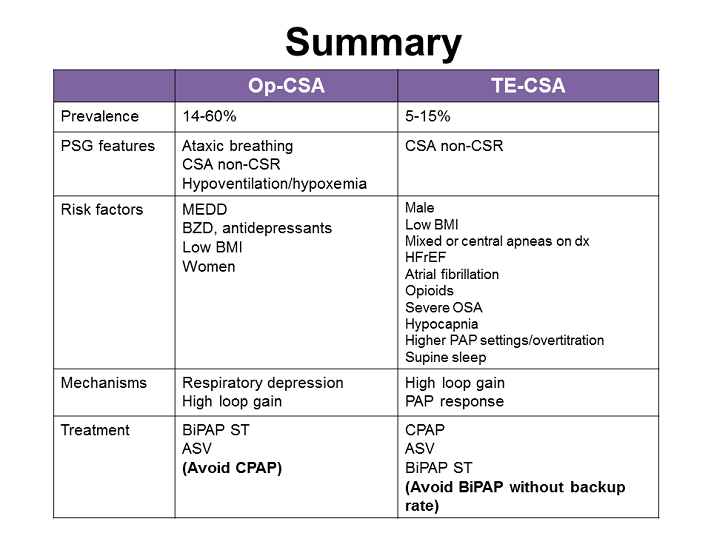
FIG. 51: This Figure summarizes the commonalities and differences between CSA that is opioid-induced and CSA that is treatment related. TE-CSA is relatively rare, and more often than not it tends to resolve by itself over time. Op-CSA, on the other hand, is quite common in chronic opioid users and should be looked for.
The polysomnographic features of both are slightly different. Ataxic breathing occurs more commonly during Op-CSA. In terms of risk factors, for Op-CSA the dose of the opioid increases the severity; women seem to be more frequently affected, as well as patients with lower BMIs.
Patients with lower BMIs also tend to be more affected with TE-CSA, but it is men who are at higher risk of TE-CSA. There are many comorbidities that appear to predispose to TE-CSA. High loop gain may be part of or the only reason for Op-CSA, as well as TE-CSA, but in Op-CSA there is the added complexity of a respiratory depressive effect, and in TE-CSA the PAP response must be considered.
In terms of treatment recommendations in Op-CSA ,CPAP therapy should be avoided, as CPAP may worsen SBD. Instead, physicians should try BiPAP ST, or ASV therapy. In TE-CSA, on the other hand, the majority of patients will resolve on CPAP therapy, which is the primary intervention recommended. If CPAP fails, ASV or BiPAP ST can be tried, but BiPAP without a backup rate should be avoided.
The clinical significance of both of these syndromes remains unknown. While we search for optimal therapies for these different breathing patterns, we do not know whether treatment is advantageous. If we learned anything from the SERVE-HF study,[12] it was that normalizing breathing during sleep in certain conditions is not always beneficial. Thus what are needed are long-term outcome studies that reveal whether treating these types of CSAs are beneficial. It might be that the situation is the opposite, that there is a survival advantage to high loop gain and some metabolic advantage for the fluctuating PCO2 and PO2 levels. At this time the consensus favors treating the breathing disorder, especially if the patient is symptomatic, and there is some evidence to guide us when choosing that treatment and that PAP modality, while we await further information.
References
Correa D, Farney RJ, Chung F, et al. Chronic opioid use and central sleep apnea: a review of the prevalence, mechanisms, and perioperative considerations. Anesth Analg. 2015;120:1273–1285.
Teichtahl H, Prodromidis A, Miller B, et al. Sleep-disordered breathing in stable methadone programme patients: a pilot study. Addiction 2001;96:395–403.
Wang D, Teichtahl H, Drummer O, et al. Central sleep apnea in stable methadone maintenance treatment patients. Chest 2005;128:1348–1356.
Walker JM, Farney RJ, Rhondeau SM, et al. Chronic opioid use is a risk factor for the development of central sleep apnea and ataxic breathing. J Clin Sleep Med. 2007;3:455–461.
Webster LR, Choi Y, Desai H, et al. Sleep-disordered breathing and chronic opioid therapy. Pain Med. 2008;9:425–432.
Mogri M, Desai H, Webster L, et al. Hypoxemia in patients on chronic opiate therapy with and without sleep apnea. Sleep Breath. 2009;13:49–57.
Sharkey KM, Kurth ME, Anderson BJ, et al. Obstructive sleep apnea is more common than central sleep apnea in methadone maintenance patients with subjective sleep complaints. Drug Alcohol Depend 2010;108:77–83
Jungquist CR, Flannery M, Perlis ML, Grace JT. Relationship of chronic pain and opioid use with respiratory disturbance during sleep. Pain Manag Nurs. 2012;13:70–79.
Farney RJ, McDonald AM, Boyle KM, et al. Sleep disordered breathing in patients receiving therapy with buprenorphine/naloxone. Eur Respir J. 2013;42:394–403.
Burgess KR. New insights from the measurement of loop gain in obstructive sleep apnoea. J Physiol. 2012;590:1781–1782.
White DP. Pathogenesis of obstructive and central sleep apnea. Am J Respir Crit Care Med. 2005;172:1363–70.
Cowie MR, Woehrle H, Wegscheider K, et al. Adaptive servo-ventilation for central sleep apnea in systolic heart failure. N Engl J Med. 2015;373:1095–1105.
Farney RJ, Walker JM, Cloward TV, Rhondeau S. Sleep-disordered breathing associated with long-term opioid therapy. Chest 2003;123:632–639.
Farney RJ, Walker JM, Boyle KM, et al. Adaptive servoventilation (ASV) in patients with sleep disordered breathing associated with chronic opioid medications for non-malignant pain. J Clin Sleep Med. 2008;4:311–319.
Javaheri S, Malik A, Smith J, Chung E. Adaptive pressure support servoventilation: a novel treatment for sleep apnea associated with use of opioids. J Clin Sleep Med. 2008;4:305–310.
Alattar M, Scharf S. Opioid-associated central sleep apnea: a case series. Sleep Breath. 2009;13:201–206.
Ramar K, Ramar P, Morgenthaler T. Adaptive servoventilation in patients with central or complex sleep apnea related to chronic opioid use and congestive heart failure. J Clin Sleep Med. 2012;8:569–576.
Javaheri S, Harris N, Howard J, Chung E. Adaptive servoventilation for treatment of opioid-associated central sleep apnea. J Clin Sleep Med. 2014;10:637–643.
Troitino A, Labedi N, Kufel T, El-Solh AA. Positive airway pressure therapy in patients with opioid-related central sleep apnea. Sleep Breath. 2014;18:367–373.
.
Reddy R, Adamo D, Kufel T, et al. Treatment of opioid-related central sleep apnea with positive airway pressure: a systematic review. J Opioid Manag. 2014;10:57–62.
Guilleminault C, Cao M, Yue HJ, Chawla P. Obstructive sleep apnea and chronic opioid use. Lung 2010;188:459–468
Cao M, Cardell CY, Willes L, et al. A novel adaptive servoventilation (ASVAuto) for the treatment of central sleep apnea associated with chronic use of opioids. J Clin Sleep Med. 2014;10:855–861.
Morgenthaler TI, Kagramanov V, Hanak V, Decker PA. Complex sleep apnea syndrome: is it a unique clinical syndrome? Sleep 2006;29:1203–1209.
Younes M, Ostrowski M, Atkar R, et al. Mechanisms of breathing instability in patients with obstructive sleep apnea. J Appl Physiol (1985). 2007;103:1929–1941.
Eckert DJ, Jordan AS, Merchia P, Malhotra A. Central sleep apnea: pathophysiology and treatment. Chest 2007;131:595–607.
American Academy of Sleep Medicine . International Classification of Sleep Disorders, 3rd ed. Darien, IL: American Academy of Sleep Medicine; 2014.
Lehman S, Antic NA, Thompson C, et al. Central sleep apnea on commencement of continuous positive airway pressure in patients with a primary diagnosis of obstructive sleep apnea-hypopnea. J Clin Sleep Med 2007;3:462–466.
Javaheri S, Smith J, Chung E. The prevalence and natural history of complex sleep apnea. J Clin Sleep Med. 2009;5:205–211.
Cassel W, Canisius S, Becker HF, et al. A prospective polysomnographic study on the evolution of complex sleep apnoea. Eur Respir J. 2011;38:329–337.
Dellweg D, Kerl J, Hoehn E, et al. Randomized controlled trial of noninvasive positive pressure ventilation (NPPV) versus servoventilation in patients with CPAP-induced central sleep apnea (complex sleep apnea). Sleep. 2013;36:1163–1171.
Dernaika T, Tawk M, Nazir S, et al. The significance and outcome of continuous positive airway pressure-related central sleep apnea during split-night sleep studies. Chest. 2007;132:81–7.
Kuzniar TJ, Pusalavidyasagar S, Gay PC, Morgenthaler T. Natural course of complex sleep apnea—a retrospective study. Sleep Breath. 2008;12:135–139.
Loewen A, Ostrowski M, Laprairie J, Atkar R, Gnitecki J, Hanly P, Younes M. Determinants of ventilatory instability in obstructive sleep apnea: inherent or acquired? Sleep 2009;32:1355–1365.
Salloum A, Rowley JA, Mateika JH, et al. Increased propensity for central apnea in patients with obstructive sleep apnea: effect of nasal continuous positive airway pressure. Am J Respir Crit Care Med 2010;181:189–193.
Stanchina M, Donat W, Corrao W, et al. Clinical use of loop gain measures to determine CPAP efficacy in patients with complex sleep apnea: a pilot study, Ann Am Thoracic Soc. 2015,12:1351-1357.
Nakazaki C, Noda A, Yasuda Y, et al. Continuous positive airway pressure intolerance associated with elevated nasal resistance is possible mechanism of complex sleep apnea syndrome. Sleep Breath. 2012;16:747–752.
Nakazaki C, Noda A, Yasuda Y, et al. Continuous positive airway pressure intolerance associated with elevated nasal resistance is possible mechanism of complex sleep apnea syndrome. Sleep Breath. 2012;16:747–752.
Montesi SB, Bakker JP, Macdonald M, et al. Air leak during CPAP titration as a risk factor for central apnea.. J Clin Sleep Med. 2013;9:1187–1191.
Guilleminault C, Simmons FB, Motta J, et al. Obstructive sleep apnea syndrome and tracheostomy. Long-term follow-up experience. Arch Intern Med. 1981;141:985–988.
Johnson KG, Johnson DC. Bilevel positive airway pressure worsens central apneas during sleep. Chest 2005;128:2141–2150.
Allam JS, Olson EJ, Gay PC, Morgenthaler TI. Efficacy of adaptive servoventilation in treatment of complex and central sleep apnea syndromes. Chest. 2007;132:1839–1846.
Morgenthaler TI, Gay PC, Gordon N, Brown LK. Adaptive servoventilation versus noninvasive positive pressure ventilation for central, mixed, and complex sleep apnea syndromes. Sleep. 2007;30:468–475.
Morgenthaler TI, Kuzniar TJ, Wolfe LF, et al. The Complex Sleep Apnea Resolution Study: a prospective randomized controlled trial of continuous positive airway pressure versus adaptive servoventilation therapy. Sleep. 2014;37:927–934