Rader - Figure 30 - Pedigree: Genotyping results Text
Rader - Figure 30 - Pedigree: Genotyping results
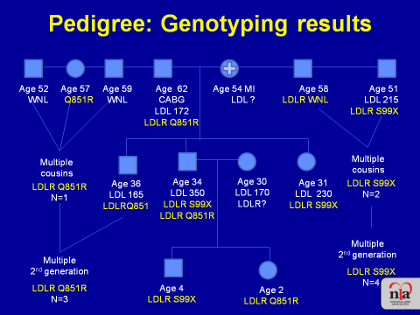
Following placement of the 2 mutations in the patient's pedigree, shown in the previous Figure, it was now possible to go into his family and rather than sequencing the entire genome, the clinician can simply genotype for these two mutations in the rest of the family to try to put the story together and identify the carriers of the mutations. As shown in this Figure, the pedigree with the genotyping results in the family highlights a couple of key points:
First, the patient's father, with an LDL-C level of 172 mg/dL, has the LDL receptor missense mutation Q851R, the one that is the less severe mutation. Thus he has heterozygous FH even though his LDL-C was not completely diagnostic of this condition. It was not possible to obtain his deceased mother's sequence, but from his father's result we can be fairly sure that his mother must have been a carrier of the premature truncation mutation, the S99X. That mutation is more severe, completely obliterates LDL receptor activity, and presumably resulted in severe heterozygous FH and her early coronary disease resulting in her death from MI.
In addition, the sequencing results shown in the pedigree show that among the father's siblings his two brothers have no mutation but his sister is a carrier of the Q851R mutation and that that mutation is also seen in the first and second generations of that side of the family. On the other side of the family, the mother's one brother also carries the LDL receptor S99X stop mutation, has an elevated LDL-C level (215 mg/dL), and although he does not currently have coronary disease, he certainly should be considered at high risk and treated aggressively. That mutation is also carried by other multiple members of that extended family who are also at high risk due to this mutation.
Finally, looking at the proband's siblings, his brother carries the RQ851 mutation, his sister is a carrier of the S99X mutation, and of his two children, one is a carrier of the S99X mutation and the other of the missense mutation.
In sum, this pedigree now shows us that this patient actually has two different mutations of the LDL receptor:
- one, LDLR S99X, is quite severe and completely knocks out the function
of the protein, causing
severe heterozygous FH in the individuals carrying this mutation; - the other, LDLR RQ851, is milder mutation that causes only mild heterozygous FH in the
individuals carrying this mutation.
Because he has both mutations, this patient is more severely affected than classic heterozygous FH, but because one mutation is "mild" he is less severely affected than classic homozygous FH. The different LDL-C levels in the family members are explained once sequencing revealed which of the two mutations they have.