|
||
|
The Journal of Nurse Practitioners
|
Jane Kapustin, PhD, CRNP - Figure 15
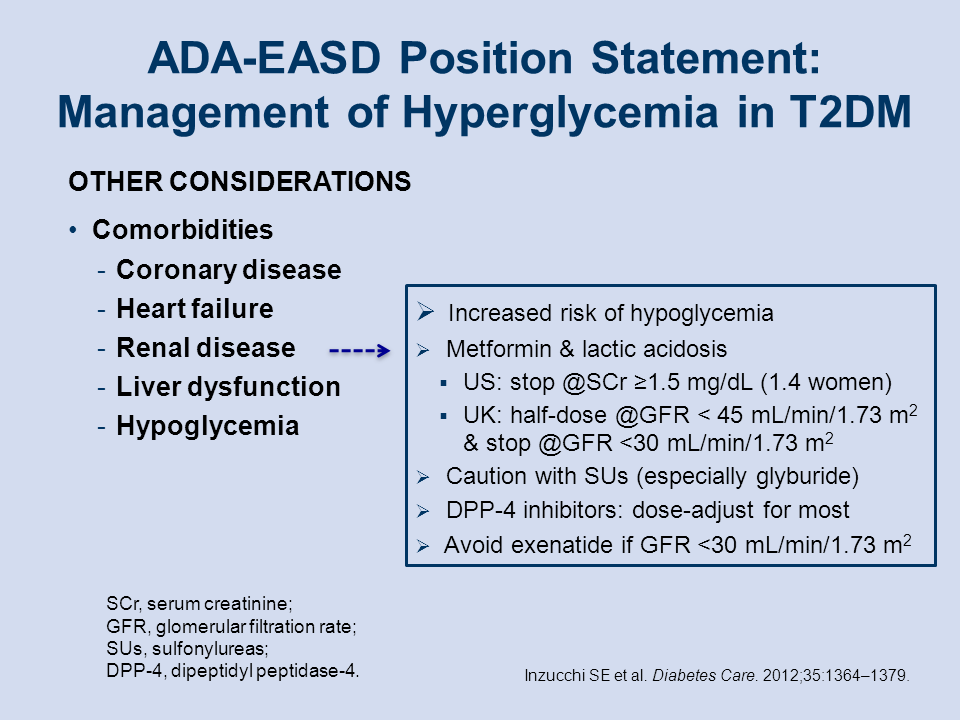
Management of Hyperglycemia in T2DM: Comorbidities: Renal disease
Another consideration in treatment in T2DM is renal disease. People with kidney dysfunction are at increased risk of hypoglycemia.[2] Renal disease or kidney dysfunction, as suggested by a serum creatinine level of ≥1.5 mg/dL in men or ≥1.4 mg/dL in women, is a contraindication to initiating or continuing treatment with metformin because of the (small) risk of lactic acidosis. The same is true for the sulfonylureas, especially one of the stronger ones, ie, glyburide (also known as glibenclamide). All the DPP-4 inhibitors (the “gliptins”) require careful dose adjustment in patients with renal insufficiency, generally reduction by half. One exception, linagliptin, has a primarily non-renal route of excretion and can therefore used without dose adjustment in patients with renal impairment. Finally GLP-1 agonists such as exenatide should be avoided if the glomerular filtration rate (GFR) is <30 mL/min/1.73 m2, and treatment with SGLT-2 inhibitors should not be initiated or continued if the GFR is significantly <45 mL/min/1.73 m2. Kapustin J. J Nurse Pract. 2014; 00:00 – 00.
References
Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes: A patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2012;35:1364-1379.