|
||
|
The Journal of Nurse Practitioners
|
Jane Kapustin, PhD, CRNP - Figure 2
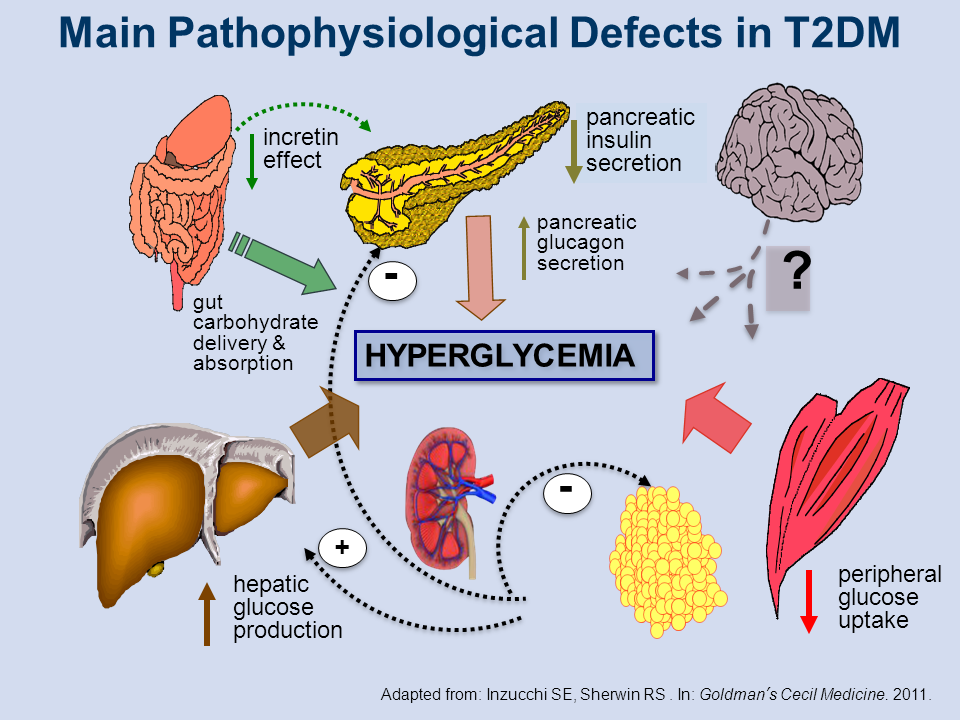
Main Pathophysiological Defects in T2DM
All of us no doubt understand that as T2DM progresses, pancreatic insulin secretion diminishes in association with β-cell apoptosis, or cell death, but less well understood, perhaps, is that at the same time as the β-cells are dying, pancreatic production of glucagon secretion is increasing. Thus even though people with T2DM are hyperglycemic, their glucose production remains relatively stable; glucagon increases, hepatic glucose production increases, and peripheral glucose uptake diminishes. The result is insulin resistance, the well-known pathophysiologic defect in patients with T2DM.
Less well known may be the role of the kidney in patients with T2DM. Numerous studies have shown that renal reabsorption of glucose is inappropriately high in T2DM, making this another main defect in this disease, in addition to lipotoxicity, glucotoxicity, and chronic oxidative stress.
Among other defects, as shown in Figure 2,[1] is a decreased incretin effect, which is seen in the way carbohydrates are delivered, absorbed, and digested in the gut, all of which are affected by the decreased incretin effect.
Finally, for patients with T2DM the neurologically controlled “satiety” response is affected, which impinges on the way people “feel full” and which is especially important for a disease where diet is so important. Kapustin J. J Nurse Pract. 2014; 00:00 – 00.
References
Inzucchi SE, Sherwin RS. Type 2 diabetes mellitus. In: Goldman L, Schafer AL, eds. Goldman’s Cecil Medicine. 24th ed. Philadelphia, PA: Saunders (Elsevier); 2011:chap 267.