|
||
|
The Journal of Nurse Practitioners
|
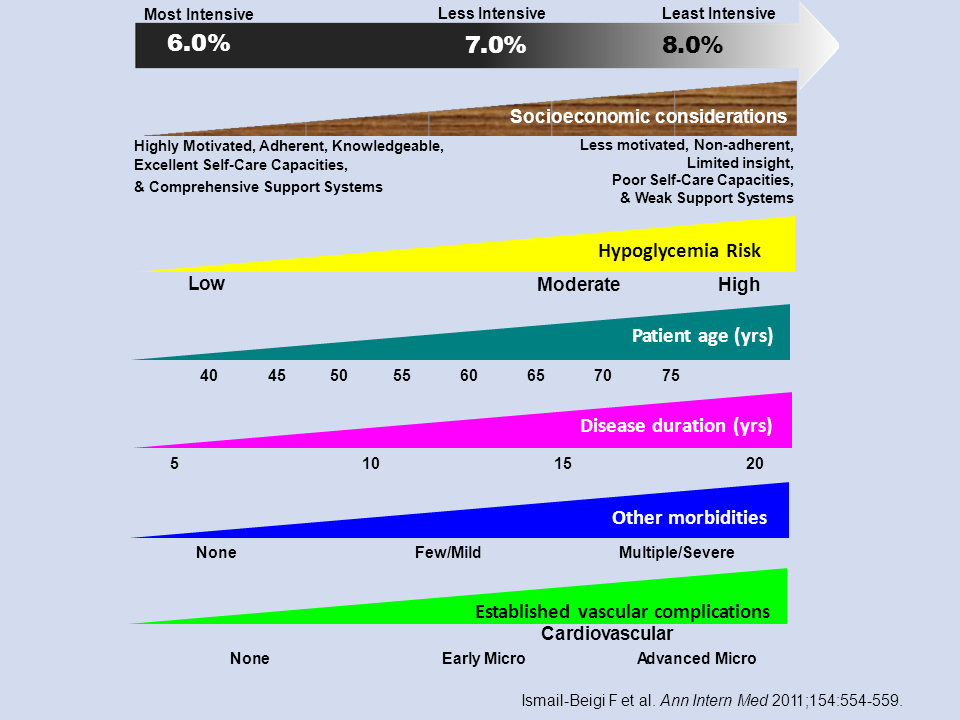
Jane Kapustin, PhD, CRNP - Figure 7
Treatment Goals for Therapy for T2DM
What about the treatment goals for therapy in patients with T2DM? One of the most frequently asked questions concerns where a patient’s HbA1C level should be maintained. As seen on left-hand side of Figure 7, the most intensive HbA1C treatment goal is around 6%; a less intensive or more moderate approach would be around 7%; and the least intensive would be 8%.[3] The rest of the Figure concerns the variables that clinicians should consider in deciding upon where to target the intensiveness of a given patient’s treatment.
Starting with the most intensive treatment goal, this means keeping a patient’s HbA1C level considerably below 7%, down around 6%. This would be reserved for highly motivated, adherent, knowledgeable patients, in other words, patients who have good self-management and a lot of support systems in place to maintain adherence with their treatment. These patients represent low hypoglycemic risks because they are able to manage their own treatment modalities. In practice this probably means that this treatment category would be reserved for patients who are at the younger end of their lifespan and have only had the disease for a few years, usually <10 years. These patients would have few comorbidities, if any at all, and no established vascular complications.
At the other end of the spectrum, the least intensive HbA1c goals would be for the patients who are less motivated, who may have limited eyesight, who are at the high end of hypoglycemic risk – they may live alone, for example – in short, patients who may have very limited support systems in general and in whom it is important not to risk hypoglycemic episodes. These patients would probably be older, have had this disease for a longer period of time, and might not be able to sense when they have a hypoglycemic event coming, ie, be “hypoglycemia unaware”. They probably have comorbidities and fairly well-established vascular disease elements, such as advanced micro- or even macrovascular complications, and for these patients an HbA1c level of <8% would probably be sufficient.
Overall, the goal is to adjust treatment intensiveness to the situation of the patients in front of us, realizing that this still allows a lot of latitude in terms of setting therapeutic goals. Kapustin J. J Nurse Pract. 2014; 00:00 – 00.
References
Ismail-Beigi F, Moghissi E, Tiktin M, et al. Individualizing glycemic targets in type 2 diabetes mellitus: implications of recent clinical trials. Ann Intern Med. 2011;154:554-559.