|
||
|
The Journal of Nurse Practitioners
|
Jane Kapustin, PhD, CRNP - Figure 5
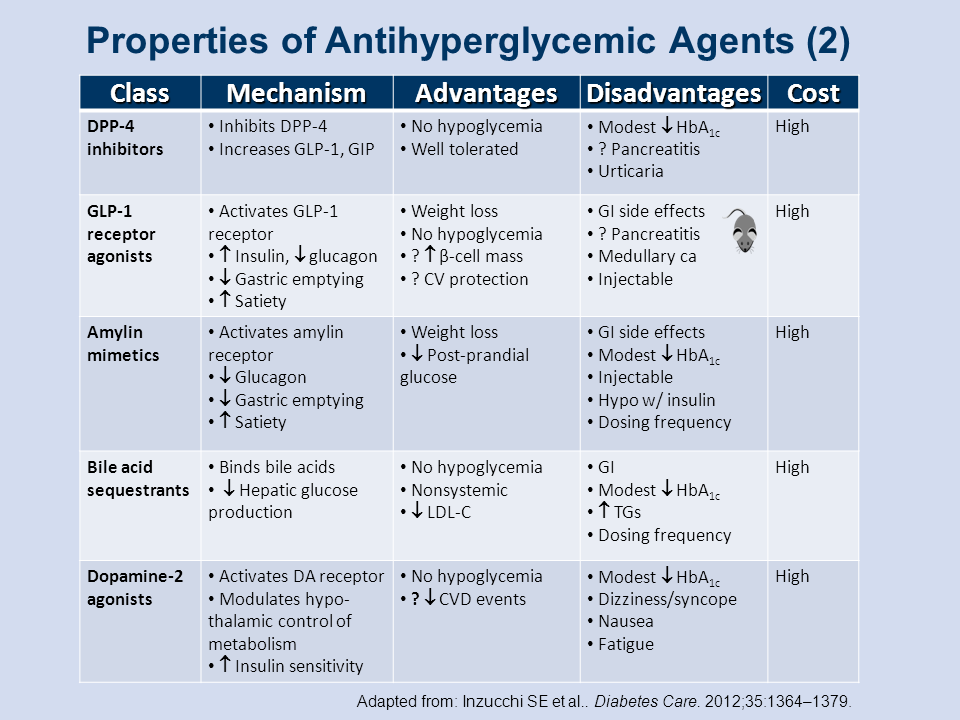
Properties of Antihyperglycemic Agents (2)
The first two classes of drugs listed in Figure 5 address physiologic postprandial insulin release stimulated by gut-derived hormones known as incretins.[2]
The first class, dipeptidyl peptidase-4 (DPP-4) inhibitors, or "gliptins," inhibits the enzymatic effects of DPP-4 and prolongs the effects of the two predominant insulin-release stimulating hormones (incretins) in the gut: glucose-dependent insulinotropic polypeptide, also known as gastric inhibitory polypeptide (GIP), and glucagon-like peptide-1 (GLP-1). The advantages of DPP-4 inhibitors are that they are weight-neutral, probably will not produce hypoglycemic effects, and are fairly well tolerated by patients. In addition to one clear disadvantage, an association with pancreatitis, this class of drugs is also associated with only a modest HbA1C lowering effect and some urticaria reported in post-marketing studies. Finally DPP-4 inhibitors are a high-cost medication.
The other class of postprandial insulin release stimulators includes the GLP-1 receptor agonists. These agents have a variety of effects, including increasing insulin secretion, lowering glucagon secretion, lowering gastric emptying, and increasing overall feelings of satiety, the latter effect leading to one of its clear-cut advantages: GLP-1 receptor agonists may induce some weight loss in patients. Other advantages include very little hypoglycemia and a suggestion that this drug class may help stabilize pancreatic β-cells so that there is less β-cell loss than with other drugs and it has been suggested that there may actually be an increase β-cell mass. There may also be some possibility of cardiovascular protection associated with these drugs.
Among the disadvantages with GLP-1 agonists are gastrointestinal side effects; some patients have intractable nausea and vomiting, which may lead to discontinuation of the medication. There may also be an association with pancreatitis and possibly with medullary cancer of the thyroid. Unlike the DPP-4 inhibitors, these drugs are all injected, which may inhibit patient acceptance, but like the DPP-4s, the GLP-1 agonists are in the high-cost category.
The third class of drugs listed in Figure 5 is the amylin mimetics. These agents are associated with some of the same mechanisms of action in terms of decreasing glucagon, helping to decrease postprandial glucose levels, and lowering or slowing gastric emptying, thus increasing feelings of satiety, which is associated with some weight loss. There is a modest HbA1C reduction with this class of drugs, but the gastrointestinal side effects may overshadow the HbA1C effects. Finally, the amylin mimetics are injectable, require dosing at mealtime, ie, 3 times a day, and again, the costs associated with this drug class are high.
Bile-acid sequestrants help decrease hepatic glucose production by binding with hepatic bile acids. A clear advantage with this class is that there is no associated hypoglycemia, its effects are nonsystemic, and there is some lowering of LDL-cholesterol levels. At the same time, this drug category has some important disadvantages. Most patients with type 2 diabetes have high triglycerides, and if a patient’s triglycerides are >500 mg/dL this medication will be contraindicated. Dosing frequency is up to 6 times per day, which may mean that patients are less compliant with the drug, and it is associated with only a modest (0.5%) HbA1C reduction. Finally the cost again counts as high.
The last category of drugs in Figure 5 is the dopamine-2 agonists. These agents bind to dopaminergic receptors to modulate hypothalamic control of dopamine metabolism, but the mechanism of action is somewhat idiopathic and so the exact physiologic mechanism is not well understood. These agents improve insulin sensitivity with no associated hypoglycemia, which is a clear advantage of this class, and there may be some lowering of cardiovascular events overall. There is a modest HbA1C reduction, about 0.5%, with some associated side effects such as dizziness, syncope, nausea, and some fatigue. Finally, because this is a fairly new class of medications, the cost can be quite high. Kapustin J. J Nurse Pract. 2014; 00:00 – 00.
References
Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes: A patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2012;35:1364-1379.